To be given as intravenous infusion over 1 hour.
A course of treatment with ZOVIRAX IV for infusion usually lasts 5 days, but this may be adjusted according to the patient's condition and response to therapy. Treatment for herpes encephalitis usually lasts 10 days.
The duration of prophylactic administration of ZOVIRAX IV for infusion is determined by the duration of the period at risk.
Adults: Treatment of herpes simplex: Obese patients should be dosed at the recommended adult dose using ideal body weight, rather than actual body weight.
Patients with herpes simplex (except herpes encephalitis) should be given aciclovir IV for infusion in doses of 5 mg/kg body weight every eight hours if renal function is not impaired.
Patients with herpes encephalitis should be given aciclovir IV for infusion in doses of 10 mg/kg body weight every eight hours provided renal function is not impaired.
Prophylaxis of herpes simplex in immune-compromised patients: Obese patients should be dosed at the recommended adult dose using ideal body weight, rather than actual body weight.
Refer to adult dosing recommendations for the treatment of herpes simplex with ZOVIRAX IV for infusion.
Treatment of varicella and herpes zoster: Obese patients should be dosed at the recommended adult dose using ideal body weight, rather than actual body weight.
Patients with varicella zoster infections should be given aciclovir IV for infusion in doses of 5 mg/kg body weight every eight hours if renal function is not impaired.
Immune-compromised patients with varicella zoster infections should be given aciclovir IV for infusion in doses of 10 mg/kg body weight every eight hours provided renal function is not impaired.
Infants and children: The dose of ZOVIRAX IV for infusion for infants and children aged between 6 months and 12 years is calculated on the basis of body surface area.
Children with herpes simplex infections should be given ZOVIRAX IV for infusion in doses of 250 mg per square metre body surface area every 8 hours for 7 days if renal function is not impaired.
In immune-compromised children with varicella zoster infections 500 mg/m
2 over a 1 hour period every 8 hours for 7 days.
For children in 6 months to 12 years with herpes simplex encephalitis, more accurate dosing is achieved by infusing 500 mg/m
2 at a constant rate over at least 1 hour every 8 hours for 10 days.
Infants and children with impaired renal function require an appropriately modified dose, according to the degree of impairment.
Elderly: The possibility of renal impairment in the elderly must be considered and the dosage should be adjusted accordingly (see Renal Impairment in the following text).
Adequate hydration should be maintained.
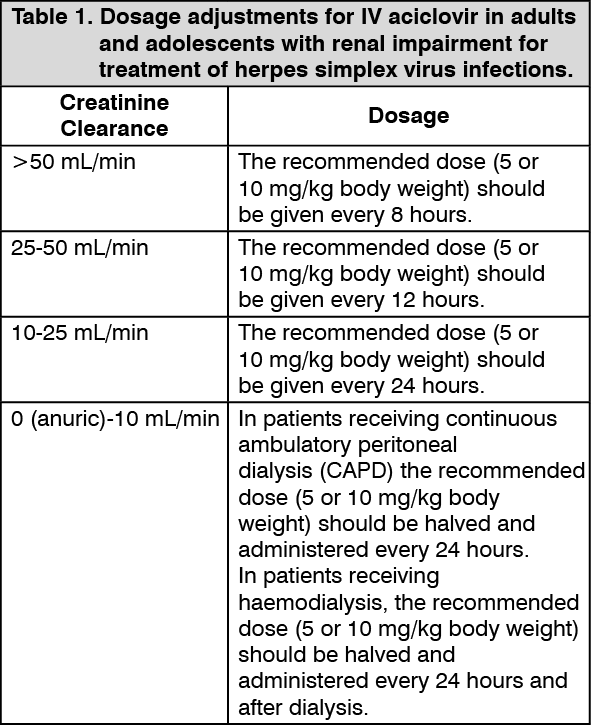
Renal Impairment: Caution is advised when administering ZOVIRAX IV for infusion to patients with impaired renal function. Adequate hydration should be maintained.
Dosage adjustment for patients with renal impairment is based on creatinine clearance, in units of mL/min for adults and adolescents and in units of mL/min/1.73 m
2 for infants and children less than 13 years of age. The following adjustments in dosage are suggested: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out